32
PARENTERÁLNÍ VÝŽIVA: JSOU DŮVODY K NÁVRATU? Pavel Těšínský MJIP, II. interní klinika 3. LF UK a FNKV, Praha kongres ČSARIM, Zlín, 9.9.2010

PARENTERÁLNÍ VÝŽIVA:
JSOU DŮVODY K NÁVRATU?
Pavel Těšínský
MJIP, II. interní klinika
3. LF UK a FNKV, Praha
kongres ČSARIM, Zlín, 9.9.2010

Korelace mezi kumulativní negativní energetickou
bilancí a infekčními komplikacemi
Villet et al.,Clin Nutr 2005;24:502-9

Je EN ve srovnání s PN u kriticky nemocných
dospělých pacientů spojena s lepším výsledkem
než PN?
Doporučení
Na podkladě 1 studie úrovně 1 a 12 studií úrovně
2 se u kriticky nemocných důrazně doporučuje
použití enterální výživy nad PN.
ALE:
Je to opravdu tak? Je každý pacient plně živený
enterální cestou?
Crit Care Med 2009 Vol. 37, No. 5
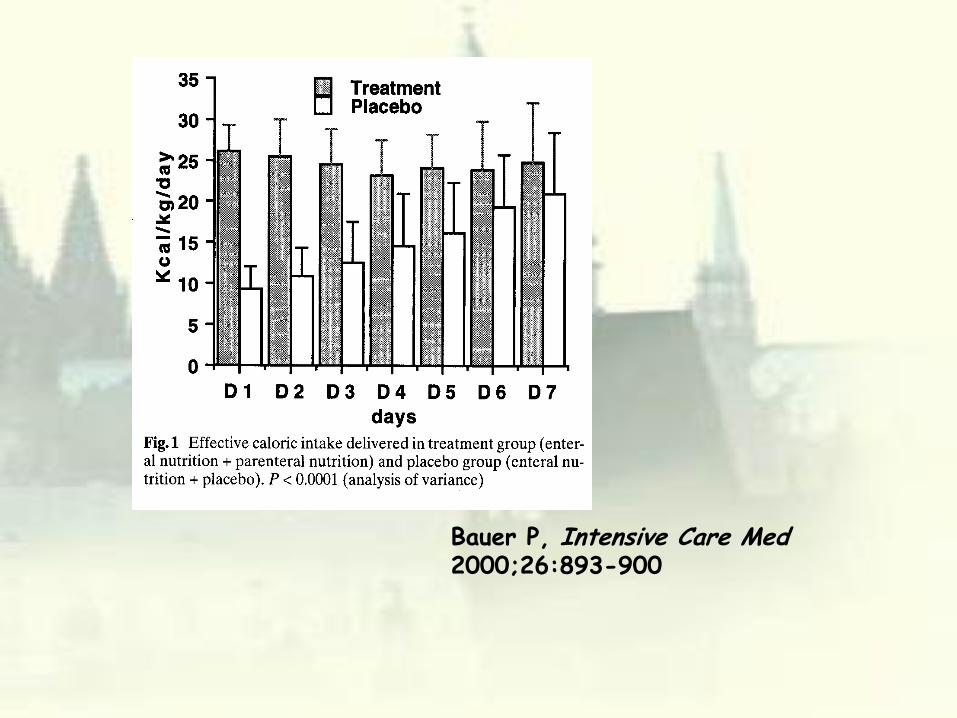
Bauer P, Intensive Care Med 2000;26:893-900

TPN: důvody k nemilosti- Nedostatečné znalosti, kompozice přípravy, obava z NÚ
- složitá logistika
- cena
- není stimulována tvorba hormonů GIT
- nižší anabolický efekt
- imunosuprese lipidy v TP
- virulentnější intestinální mikroflora
- hyperglykemie
- deficience Gln
- atrofie GALT
- infekční morbidita
- a mnohé další

Improving Nutrition CareLindorff Larsen et al. Clin. Nutr. 2007

KOMPLIKACE PN KOMPLIKACE EN
• hyperglykemie
• metabolické poruchy
• infekce
• komplikace
venosního přístupu
• cholestaza
• steatosa
• hyperglykemie?
• metabolické poruchy
• průjem
• zvracení, aspirace
• komplikace sondy
• abdominální distenze
• netolerance

TPN vs. EN:
vliv na infekční komplikaceSimpson et al, CCM 2005; 31: 12-23

TPN vs. EN:
vliv na mortalitu
Simpson et al, CCM 2005; 31: 12-23

Peter JV et al: A meta analysis of treatment outcomes
of early enteral versus early parenteral nutrition in
hospitalized patients (CCM 2005; 33: 213)

Mortalita: EEN vs. EPN: bez rozdílu

American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.) Board of
Directors
Clinical Guidelines for the Use of Parenteral and Enteral Nutrition in
Adult and Pediatric Patients, 2009
JPEN J Parenter Enteral Nutr 2009 33: 255-259
ZAČÍT S TPN DŘÍVE?
GUIDELINES USA/CDN:
• pokud EEN proveditelná v průběhu
prvních 7 dnů, není indikováno zahájení
žádné zvláštní nutriční terapie (C)
• pacienti dosud zdraví: zahájit TPN po 7
dnech (E)
• pacienti v malnutrici: zahájit TPN ASAP
(C)

ZAČÍT S TPN DŘÍVE?
GUIDELINES ESPEN:
• všichni pacienti, u nichž se neočekává
normální výživa během 3 dnů, mají dostat
PN během 24-48 hod., pokud netolerují
EN nebo je EN kontraindikována (C)
• všichni pacienti, u nichž není dosaženo
cílové dávky EN po 2 dnech, jsou
indikováni k suplementární PN (C)

SOUHRN PRO PN,
ASPEN i ESPEN
• PN should be prescribed when enteral feeding is failing, as alternative or complementary therapy to reach energy requirements
• Carbohydrates should not be administered in too much quantity
• Lipid emulsions including MCTs/olive oil/fish oil should be considered
• AA should include Alanyl-Glutamine
• Micronutrients should be included

LIPIDY v PN ASPEN, 02/2009
• IV lipids are an integral part of PN as an energy source and provide essential fatty acids in long term ICU patients
Grade C
• LCT/MCTs, olive oil based, fish oil enriched emulsions show clinical advantages over omega 6 fatty acids emulsions (except in terms of survival)
Grade B
AMINOKYSELINY A MIKRONUTRIENTY
• Amino acids should be provided at the level of 1.3 to 1.5
g/kg/day if energy balance is optimized
Grade B
• The Amino Acid solution should include 0.2 to 0.4 g/Kg
BW/Day of glutamine (0.3 to 0.6 g/Kg BW/ day alanyl-
glutamine) Grade A
• Any PN prescription should include 1 daily dose of
multivitamins and 1 daily dose of trace elements
Grade C

PŘEDOPERAČNÍ PN
• In severely undernourished patients who cannot be
adequately orally or enterally fed (Grade A).
SACHARIDY PŘEDOPERAČNĚ• For most patients preoperative carbohydrate loading
using the oral route is recommended (Grade A).
• In the rare patients who cannot eat or are not allowed to
drink preoperatively for whatever reasons the
intravenous route can be used.

POOPERAČNÍ PNIn undernourished patients in whom enteral nutrition is not
feasible or not tolerated (Grade A);
In patients with postoperative complications Unable to absorb adequate amounts of oral/ enteral feeding for at least 7 days (Grade A).
In patients who require postoperative artificial nutrition, enteral feeding or a combination of enteral and supplementary parenteral feeding is the first choice (Grade A).
Combinations of enteral and parenteral nutrition in patients in whom >60% of energy needs cannot be met via the enteral route (Grade C)
In completely obstructing lesions surgery should not be postponed because of the risk of aspiration or severe bowel distension leading to peritonitis (Grade C).
In patients with prolonged gastrointestinal failure PN is lifesaving (Grade C).

ENERGETICKÝ PŘÍJEM
• The commonly used formula of 25 kcal/kg ideal body weight (Grade B).
• Under conditions of severe stress requirements may approach 30 kcal/kg ideal body weight (Grade B).
• In illness/stressed conditions a daily nitrogen delivery equivalent to a protein intake of 1.5 g/kg ideal body weight is generally effective to limit nitrogen losses (Grade B).
• The protein/fat/glucose caloric ratio should approximate to 20:30:50% (Grade C).

GLUKOSA / LIPIDY (ESPEN 2009)
• from 50:50 to 60:40 of the non-protein
calories, due to the problems encountered
regarding hyperlipidaemia and fatty liver,
which is sometimes accompanied by
cholestasis and in some patients may
progress to non-alcoholic steatohepatitis
(Grade C).

METODIKA TPN (ESPEN 2009)
• all components of the parenteral nutrition
mix are administered simultaneously over
24 h (all-in-one or multi-bottle system)
(Grade A).

SPECIFICKÉ NUTRIENTY
(ESPEN 2009)
• The optimal PN regimen for critically ill surgical patients
should probably include supplemental n-3 fatty acids
(Grade C).
• The EB for such recommendations requires further input
from prospective randomised trials.

MIKRONUTRIENTY (ESPEN 2009)
• In well-nourished patients who recover oral or
enteral nutrition by postoperative day 5 there is
a little evidence that intravenous
supplementation of vitamins and trace elements
is required (Grade C).
• In those patients after surgery who are unable to
be fed via the enteral route, and in whom total or
near total parenteral nutrition is required, a full
range of vitamins and trace elements should be
supplemented on a daily basis (Grade C).

Pokud je PN indikovaná,
maximalizovat její efekt
• dávka, monitorace, složení, aditiva
• overfeeding je spojen s významnými komplikacemi
časně i pozdně
• permisivní underfeeding po krátkou dobu nevadí
• obesní nemocní živit na ideální hmotnost
• kontrola glykemie
• parenterální Gln
• pozor na LCT
• permanentně zkoušet a navyšovat EN s cílem převodu
na plnou EN
• stimulovat anabolismus

HOT TOPICS: glutamin
• studie do 08/2008
• IV Gln u kriticky nemocných je spojen s n.s. redukcí
mortality (RR 0.71 (95% CI 0.49, 1.03) a s mírnou
redukcí infekčních komplikací
• IV Gln snižuje riziko rozvoje MOF
• neprokázán negativní efekt IV Gln
Avenell A: Current evidence and ongoing trials on
the use of glutamine in critically-ill patients and
patients undergoing surgery. Proc Nutr Soc 2009
68(3): 261-268

HOT TOPICS: glutamin
• Scandinavian Glutamine Study
• n= 280Pts PP, 400 pts ITT
• SOFA: n.s.
• ICU mortalita: -10%
• 28d mortalita: - 8%
Werneman J, oral
communication,
ESPEN 08/2010

HOT TOPICS: Gln+Se
• SIGNET (UK, Scotland)
• n 1100pts
• GLN,Se,GLN+Se,0
• infekce: bez rozdílu pro všechny skupiny kromě Se (n.s.)
• mortalita: bez rozdílu pro všechny skupiny
Simpson WG,
oral communication, 08/2010

HOT TOPICS: lipidy v PN
• fish oil
• imunomodulační efekt závisí na dávce
• převážně chirurgicčtí pacienti
• perioperativní aplikace má větší efekt než pooperativní
• redukce LOS, doby UPV, v některých studiích nižší
mortalita.
Calder PC Proc Nutr Soc
2009; 68(3): 252-260

HOT TOPICS:
imunonutrice u chirurgicky nemocných
• Gln, antioxidanty, vitaminy, omega-3 FA, nukleotidy
• IV Gln do PN, E Gln popáleniy, trauma
• Selen asi positivní efekt u kriticky nemocných
• n-3FA ARDS
• Arg ne u sepse, ano předoperačně u neseptických v
malnutrici a u onkologicky nemocných
Xu J; Yunshi Z; Li R Curr Drug
Targets 2009; 10(8): 771-777

SOUČASNÁ PRAXE
PN indikovat poté, co byla iniciována EN
(nebo byla kontraindikována) se snahou o
maximální toleranci (prokinetika,
transpylorický přístup):
• pacient bez malnutrice / dosud
nekatabolický: pokud EN nefunguje 5-7dnů
• pacient v malnutrici: pokud nedosaženo
cílové EN do 48 (72) hod.


















