Title Herpes simplex virus infection of respiratory tract in intensive care unit Author(s) Lui, Mei-sze; –÷ ŽŠ Citation Issued Date 2012 URL http://hdl.handle.net/10722/173733 Rights Cr ea tiv e Common s: Attribution 3.0 Hong Kong Lic en se
Transcript
8/17/2019 FullText (98)
http://slidepdf.com/reader/full/fulltext-98 1/31
TitleHerpes simplex virus infection of respiratory tract in intensivecare unit
Author(s) Lui, Mei-sze;–÷ ŽŠ
Citation
Issued Date 2012
URL http://hdl.handle.net/10722/173733
Rights Creative Commons: Attribution 3.0 Hong Kong License
8/17/2019 FullText (98)
http://slidepdf.com/reader/full/fulltext-98 2/31
1
Herpes Simplex virus infection of respiratory tract in
Intensive Care Unit - a single centre experience
By
Dr Lui Mei Sze
(No: 1998256815)
This work is submitted to
Faculty of Medicine of The University of Hong Kong
In partial fulfillment of the requirements for
The Postgraduate Diploma in Infectious Diseases, PDipID (HK)
Date: 10th August 2012
Supervisor: Dr VCC Cheng
8/17/2019 FullText (98)
http://slidepdf.com/reader/full/fulltext-98 3/31
2
Declaration
I, Lui Mei Sze, declare that this dissertation represents my own work and that it has
not been submitted to this or other institution in application for a degree, diploma or
any other qualifications.
I, Lui Mei Sze also declare that I have read and understand the guideline on “What is
plagiarism?” published by The University of Hong Kong (available at
http://www.hku.hk/plagiarism/) and that all parts of this work complies with the
guideline.
Candidate: Lui Mei Sze
Signature:
Date:
10th August 2012
8/17/2019 FullText (98)
http://slidepdf.com/reader/full/fulltext-98 4/31
3
Acknowledgement
The author would like to the acknowledge the guidance and supervision from Dr
Vincent Cheng and the Department of Microbiology, Queen Mary Hospital, The
University of Hong Kong, for undertaking the study project. The author would also
like to thank Dr Chan Wai Ming and the Department of Intensive Care Unit, Queen
Mary Hospital, for the support on the study project.
8/17/2019 FullText (98)
http://slidepdf.com/reader/full/fulltext-98 5/31
4
Abstract (word count: 342 )
Background
Herpes Simplex virus (HSV) is commonly isolated from the specimen of
respiratory tract in hospitalized patients. It can indicate asymptomatic shedding
from respiratory epithelium, viral reactivation with macroscopic airway lesion, or
even pneumonia. There are significant differences in the awareness, interpretation
and management strategies of the condition among departments and hospitals.
Objective
A retrospective case review of clinical features, management and outcomes of
hospitalized subjects from whom HSV is detected in the bronchoalveolar lavage
specimen
Method
The medical records of all the patients with pneumonia and bronchoalveolar
lavage (BAL) being positive for HSV culture, who were admitted between 2004 and
2011 to Queen Mary Hospital, were retrieved from the clinical management system or
record folders. Their demographic data, laboratory results, progress and outcomes
were recorded.
Results
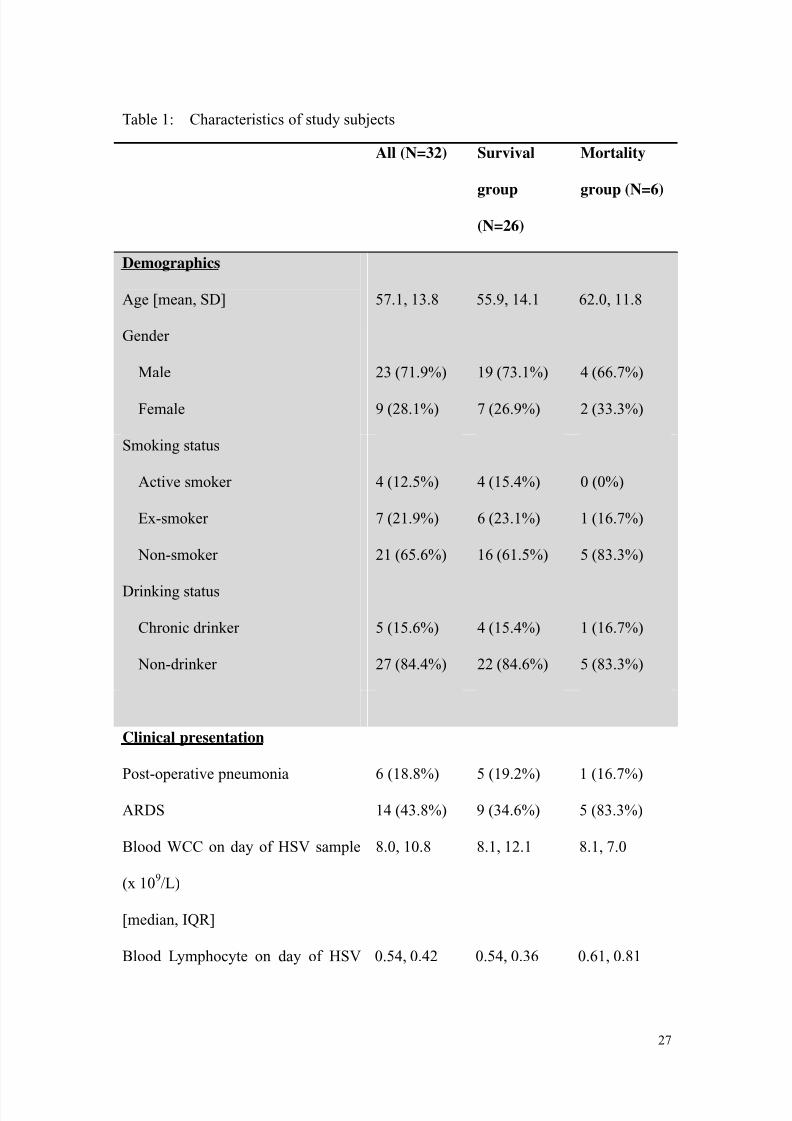
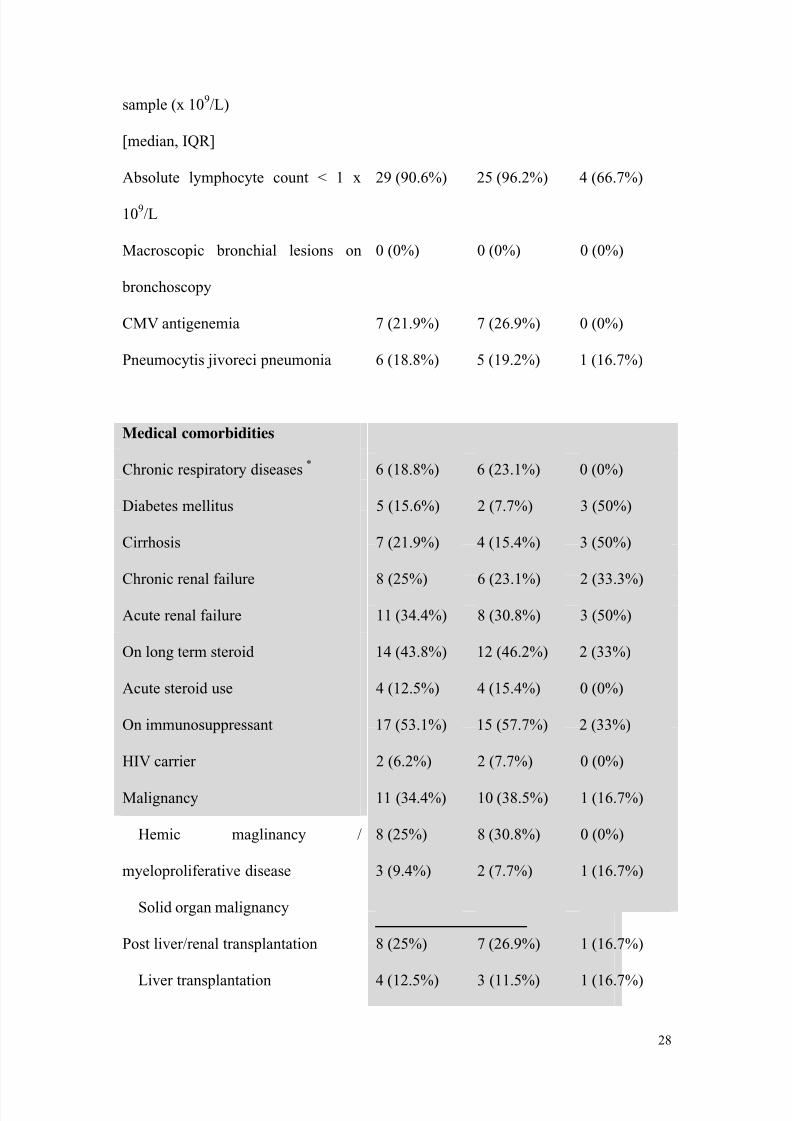
A total of 32 patients were identified over the period of seven years. 81.3% of
8/17/2019 FullText (98)
http://slidepdf.com/reader/full/fulltext-98 6/31
5
them were emergency admission while 18.8% were elective admission. Most of
them (90.6%) required admission to the Adult Intensive Care Unit. 59.3% (n=19)
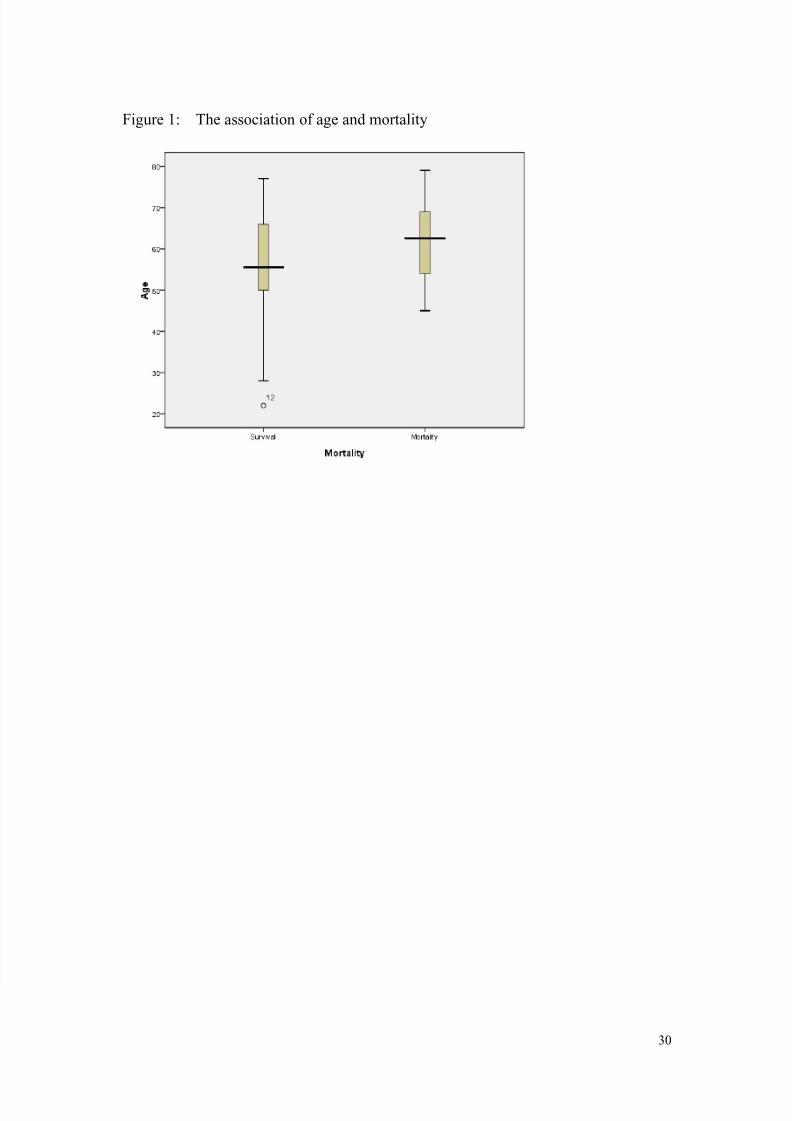
required intubation and mechanical ventilation during hospitalization. The mean age
was 57.1 (SD 13.8) year old. 71.9% were male patients. No patients with HSV
detected in BAL had macroscopic lesion on bronchoscopy. No cytological
examination on the BAL was performed. HSV reactivation is commonly associated
other opportunistic pathogens such as Pneumocystis jivoreci (21.9%) and
cytomegalovirus antigenemia (18.8%). Majority of the subjects (90.6%, n=29) with
HSV infection were lymphopenic (absolute lymphocyte count <1 x 109/L) which
could indicate underlying impairment in cell-mediated immunity related to
malnutrition, hematological disorders, use of immunosuppressants. Similar
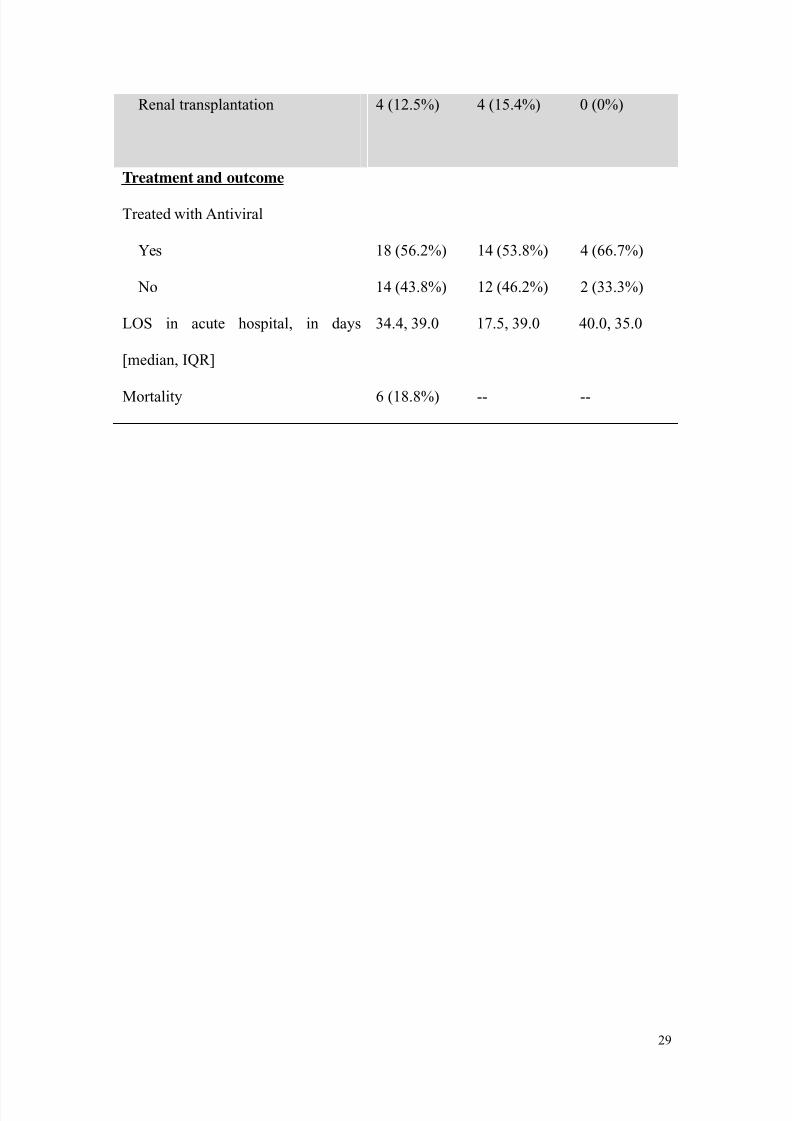
proportion in the surviving group received anti-viral treatment as compared to the
mortality group (53.8% versus 66.7%, respectively), implicating that treatment with
anti-viral medication might not have important impact on mortality rate.
Conclusion
The awareness of significance of HSV reactivation in lower respiratory tract is
highly variable. Lymphopenic patients are at high risk of HSV reactivation or HSV
pnemonitis. The presence of lymphopenia, or other immunocompromised state
8/17/2019 FullText (98)
http://slidepdf.com/reader/full/fulltext-98 7/31
6
should prompt the physicians to perform a thorough work-up for HSV infection even
in the absence of macroscopic lesions.
8/17/2019 FullText (98)
http://slidepdf.com/reader/full/fulltext-98 8/31
7
Body Text (Word count: 3109)
Background
Herpes simplex virus 1 and 2 (HSV-1 and HSV-2), also known as Human herpes
virus 1 and 2 (HHV-1 and -2), are members of the herpes virus family, Herpesviridae,
that contains double-stranded DNA. Both HSV-1 and HSV-2 are ubiquitous in
environment and contagious among human. HSVs are predominantly neurotropic, and
possess genes associated with latency in neuronal tissues after primary infection.
Majority of human has been exposed to the virus early in life, which is commonly
asymptomatic or presented as non-specific febrile illness, and shed the virus in
secretions upon reactivation in later life. HSV-1 disease primarily involves the
mouth, eye and the central nervous system. After anchoring to the receptor of
epithelial cells, the envelope of the virus fuses with the cell membrane, followed by
the transport of the viral nucleocapsids cross the cytoplasm to the nucleus of the
infected cells. Assembly of capsids and replication of viral DNA occur. Viral
glycoproteins are processed in the Golgi apparatus and incorporate into cell
membrane, from which the viral envelope is acquired as the virus buds out from the
nucleus.
Reactivation of latent HSV infection may be asymptomatic, though typically, it
gives vesicular lesions or ulcers. DNA of herpes virus passes along nerve axon to
8/17/2019 FullText (98)
http://slidepdf.com/reader/full/fulltext-98 9/31
8
the nerve ending and epithelial cells, where it gives rise to visible lesions.
Occasionally, shedding of virus may occur without symptoms or visible lesions.
Reactivation can be triggered by diverse stimuli such as sunlight, febrile diseases,
local trauma or physical stress. Common sites of HSV reactivation include
respiratory tract, eyes, oral or genital mucosa and the central nervous system.(1)
Regarding the respiratory tract, the virus could cause cold sore, gingivostomatitis,
tracheobronchitis and even pneumonia.(2) The diagnosis of HSV reactivation is
typically clinical when classical lesions are encountered, and supported by viral
detection or serological studies. Viral detection by means of culture, electron
microscopy, antigen detection by immunofluorescence, or viral DNA amplification by
PCR technique allows earlier confirmation of diagnosis compared to antibody tests.
Herpes virus was reported to be the causative pathogen of pneumonia and erythema
multiforme since 1949 (3). In subsequent decades, Herpes infection has been
repeatedly reported in case report and series as the pathogens causing
tracheobronchitis or infection of lower respiratory tract.(4-8) In intensive care
setting, HSV is commonly recognized in the respiratory tract specimen, regardless of
the presence or absence of macroscopic lesion, and the immune status of the host.(9)
Critically ill patients commonly possess risk factors for HSV reactivation, such as
systemic stress related to the critical illness, heightened stress hormone activity,
8/17/2019 FullText (98)
http://slidepdf.com/reader/full/fulltext-98 10/31
9
immunocompromised state due to organ failures or drugs, and local airway
trauma.(10) Local trauma as a result of intubation, instrumentation, mechanical
suction, burn could promote squamous metaplasia, which predispose to HSV
reactivation at the airway epithelium.(9) HSV can reach the lower respiratory tract by
aspiration of shed virus from upper respiratory tract, hematogenous spread, or
reactivation of latent infection within the vagal nerve with resultant spread to the
lung.(9) Cell mediated immunity is of paramount importance in controlling and
combating HSV reactivation, or in the other words, recurrent HSV infection could